Today, we’ve got a smattering of amazing educational opportunities to announce:
This Thursday in Bend, OR @ 7:30 at the Westside Clinic:Athletes – Please join Jay Dicharry PT (REP Biomechanics Lab Director) Matt Lieto (Pro Triathlete) and Keats McDougal (Ironman Canada & Tahoe Director) for a night of Mobility and Multi-sport discussion. Jay will provide the latest research on mobility and best practices for multisport athletes. We’ll answer the most common questions: What does stretching do for the body? When should you stretch? How long? What’s the difference between dynamic warm-up and stretching? And how does soft tissue work play into this whole discussion? Next, Matt will discuss his training plans and and upcoming race prep considerations. Matt will show you how the lessons he’s learned along the way can help you prepare better for your next event. Finally, Matt will lead a Q and A with Keats. They’ll provide an overview and considerations of these two challenging courses. It will help you prep for this year’s race, or feed your stoke for next year! Stick around after for a question and answer session with our panel. And yes, we’ll have beer. Cost: free. No brainer!
This weekend in Boulder Colorado (7/13-7/14):Calling all healthcare professionals – are you tired of getting your information on running mechanics from the mainstream media? Would you be interested in a immersive weekend of education that is based around hundreds of peer-reviewed articles, hands on clinical assessment, and gait cues? We’ll construct a framework of what we know about running mechanics and their effect on performance and economy. And more importantly, we’ll show you how this information applies not just to the masses, but to your individual patients. In short, this is all the stuff you wish they had told you in Med school, PT program, or ATC curriculum. There are still a few spots left. See here for details.
August 23-24th in San Jose:Tri-athletes and would-be coaches– are you looking to get your Level 1 certification? Then join us for the USA Triathlon coaching clinic. Two days packed full of essential knowledge to help you and your athletes succeed.
Sept 21st and 22nd in Bay Area:Running Coaches – this one is all for you. We are going to delve into the truth behind running mechanics, screening strategies for your team, the impact of strength training to improve performance, discuss the role of footwear, and more. Andrew Allden chairs this event – he’s brought in a knock out panel each and every time – Learn to think outside the box to take your team to the next level @ this USATF Level 3 Coaching Seminar. More info here
Yea, I know – blogging and tweeting is supposed to make us all smarter. But you know what really makes us smarter? talking face to face. See you soon!
There’s a good chance that you heard a friend say ” I sprain my ankles all the time”….or maybe you are the one saying this! Why do some people sprain, and then keep spraining their ankles over and over? Well, we recently published a study examining just this. This study was first-authored by one of our former grad students, Lisa Chinn, PhD, as part of her dissertation at the University of Virginia. While Lisa has moved on to a faculty position @ Kent State, she spearheaded this project. So, I thought I’d play “7 Questions with Dr. Chinn.”
I’ll briefly set the stage here. People with chronic ankle instability sprain, and keep spraining their ankles. There has been lots of attention paid to this area of research lately, because lots of sprains can cause lots of long term problems, and lead to lots of down time in training. Most of the research comparing the folks who keep spraining their ankles is done comparing walking and running barefoot. Yes, I know the barefoot movement is strong, but let’s face it – most people are wearing shoes, and despite what you’d like to think, barefoot gait is quite different than your gait in shoes (and it’s NOT just rearfoot vs forefoot folks….) Given the following, we thought that we’d examine the different ways people walk and run when they have healthy ankles, “single-sprain” ankles, or “chronic ankle instability” ankles. This got slightly technical at times, but I tried to summarize things towards the end. Since about 30-60% of you will have this issue, let’s ask Dr Chinn some Q’s:
1. What is chronic ankle instability, and how does this differ from people who have only had one sprain?
Chronic ankle instability (CAI), interestingly enough, is a very difficult (sometimes frustrating) syndrome to define. There is an ongoing discussion for a common description of CAI; however as of now, there is not a universally accepted definition. Some researchers rely purely on subjective reporting of symptoms by patients, while others, require some type of mechanical dysfunction to be present at the ankle joint, while still others desire a history of multiple ankle sprains. And of course, there are some who use any combination of the three. The majority of researchers (myself included) will described CAI as the long-term feelings of your ankle giving way or weakness following an initial ankle sprain. This can occur as a result of a single ankle sprain or from an accumulation of multiple sprains. Many subjects/patients claim to “tweak” their ankles all the time. It is estimated that about 30-60% of individuals that sustain an initial lateral ankle sprain will develop CAI.
There is a group of individuals who sprain their ankle once and who do not go on to develop CAI; researchers are currently using the term “coper” to describe these individuals. Research is relatively new on this population. What about them results in a full recovery from their ankle sprain? Was the sprain different or was something regarding their rehabilitation different? Are there other characteristics of these individuals that reduce their feeling of instability? Or, have they changed their lifestyle to not put themselves at risk for “tweaking” their ankle? This is a very exciting area of research because, our goal as a clinician is to prevent CAI from occurring and since we probably won’t ever figure out how to actually prevent ankle sprains from happening; we would like to determine how to get all ankle sprainers to become copers.
2. Why did you choose this topic to research?
I am an Athletic Trainer by profession. While working with various sports, at various levels, and multiple age groups one injury I always encountered were ankle sprains. No matter who you are, there is a risk of suffering an ankle sprain. With my background in athletic training and my exposure to the injury, when I decided to go to the University of Virginia for my doctorate I decided that I wanted to focus my research on ankle sprains and ankle instability. Being at UVA gave me access to prominent ankle researchers and an unbelievable motion analysis laboratory which I took advantage of.
This particular study was developed as a progression from a previous study conducted at the lab. A couple of years prior to my arrival to UVA, Lindsay Drewes (now Lindsay Sauer) and Patrick McKeon, conducted a similar study in CAI subjects, however, their data was collected while subjects were barefoot (Drewes et al., 2009; Drewes, McKeon, Kerrigan, & Hertel, 2009). Their studies reported some interesting findings; however asking individuals to perform barefoot tasks is novel, so I wanted to replicate the study while subjects were shod (shod means in shoes), a more common/comfortable condition.
3. What did you find?
The short answer: we found that while shod, gait kinematics are different between those with and without CAI. (note: kinematics is a fancy word for range of motion)
Interestingly, unlike previous gait research on CAI subjects, we did not find kinematic differences just prior to, at, or immediately following initial contact. I think adding shoes to our methods has revealed altered kinematics that barefoot methods had not previously done. Our kinematic differences occurred towards terminal stance as well as during swing. One thing to note is; no one really understands when ankle sprains occur, it has been hypothesized that they may occur either at initial contact OR terminal stance (Konradsen & Voigt 2002). However the majority of research has only focused on initial contact. Our study actually evaluated the entire gait cycle finding difference at terminal stance is very new and original. Hopefully this will encourage more researchers to evaluate the later stages of gait in the future.
4. Given that the previous research was using people walking/running barefoot, what do you think adding shoes into the equation helps?
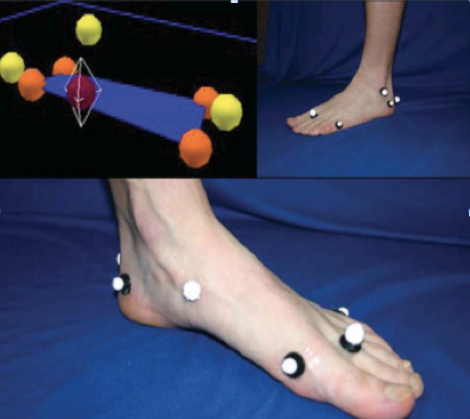
Adding shoes to the research has added a piece to the mysterious CAI puzzle. Before I discuss what shoes added, let me explain a little about the shoes we used. We were able to obtain multiple pairs (both men and women sizes) of Brook Defyance shoes. Collaborating closely with Brooks, we were able to remove various aspects of the shoe to enable us to place anatomical markers on a subject’s skin without disrupting the integrity of the shoe. Placing markers on the skin allowed us to better observe joint kinematics. Placing markers on top of shoes (which has been done in the past) only allows researchers to observe what the shoe is doing. Shoes may slip or move differently than the joint. Our goal was to see what each individual’s limb was doing, which with this custom shoe we were able to do.
So, getting back to your question, I believe incorporating shoes, specifically our custom shoes, has significantly contributed the CAI literature. Previous research has shown that there are kinematic differences and muscle activation differences between running barefoot and shod (Kerr et al 2009, De Wit et al 2000, Burkett et al 1985). If anyone has ever tried to go and run barefoot (outside or on a treadmill) without weeks of acclimation, your feet hurt and your gait naturally changes in order to adequately absorb forces. The majority of previous CAI literature asked their subjects to perform this novel task of running barefoot. Knowing that gait changes, we are unsure if their findings are due to the task or due to CAI or both. Allowing our subjects to wear shoes, we were able to capture a more natural gait stride. Secondly, plantar stimulation has been shown to affect CAI subjects differently than healthy controls. Placing shoes on our subjects may have provided some stimulation that barefoot gait does not. Plus, being an athletic trainer, I always want to try to mimic what athletes do and there are not many sports that train or compete barefoot.
5. Can you make any recommendations based on this study?
I think the most important recommendation I have for clinicians and athletes is not to shrug an ankle sprain off as “just” an ankle sprain. This study as well as the majority of CAI literature shows that individuals with CAI have both local and global alterations compared to healthy controls. We also know that CAI has been linked to osteoarthritis. This study specifically shows that gait changes can be observed. After suffering from an ankle sprain and those who have CAI should evaluate their rehabilitation and not hurry back to activity. Therapists can incorporate gait re-training exercises into rehabilitation.
6. What questions remain unanswered about the effects of CAI on athletes?
Oh so many! As any researcher will tell you, as we answer one question it seems like 10 more pop up. I touched upon this previously, but I think the three most important unanswered questions pertaining to CAI are, 1) What causes it? 2) Can we prevent it? and, 3) How do we best treat it? I know these are three very broad questions, but it’s what all CAI researchers are striving to determine.
7. Describe your new career/research interest for us?
Since leaving UVA about a year ago and starting here at Kent State University, my overall research focus has not changed; I still want to better understand CAI and determine how to prevent CAI. However, because I do not have access to a state-of-the-art motion analysis lab my methods are shifting a bit. Neuromuscular control, balance, and proprioception are, in my opinion, the keys to ankle sprain rehabilitation. I am implementing various interventions on individuals with CAI in hopes to determine the most effective way to treat this syndrome.
So…..for those of you wanting a simple summary. Here it is. People who keep spraining their ankles walk and run different from those who don’t sprain frequently. While some of you may say “who cares” – this is pretty important stuff. You see, all the gait research out there says something pretty simple. Variability is good. Its good to have slightly different ways to move. This way, when you get into “interesting situations” (like when you plant your foot slightly wrong) you have a skill set in place to correct your ankle position and save your body from injury. But this study shows that the pattern of people with CAI is different. And since these people keep spraining, one could say this compensated pattern really isn’t working….and is likely a big contributing factor to their ongoing issues.
From the clinical side, its a good idea to improve the stability of your foot and ankle. Strong muscles inside the feet means less stress to the joint and better proprioception for faster stability, which both reduce injury risk. Want some more? Check out foot some specific foot strengthening exercises in my book, and on this video below (right about 3:22).
Lastly, I’d like to say thanks to Lisa for all her work on this project, and thanks to Brooks for supplying shoes, and helping to ensure that the modifications we made to the study shoes to get 3D markers on the foot did not alter the function of the shoe during walking and running. If you’d like to contact Dr Chinn for additional questions, feel free to contact her below.
Lisa Chinn, PhD, AT. Assistant Professor in Athletic Training, Kent State University, Room 266D MACC Annex,Kent, OH 44242 – lchinn@kent.edu
Its just like the summer camp you went to as a kid. Except that……
Instead of eating hot dogs, we’ve got fully catered meals.
Instead of “being prepared” like a good Scout, we’ve got full sag on every workout.
Instead of dodgeball, we start each day with body work, strength training, or yoga.
Instead of “trying harder” to make it through the obstacle course, we’ll coach you to “move smarter” through the most efficient mechanics for your sports.
Instead of a councilor that reads comic books, your camp leaders wrote the book on training, and teach nationally.
Instead of cheesy sing-alongs, we’ll show you all the secrets to training, equipment, and recovery for you are fully prepared for every race scenario.
Instead of fruit punch, you’ll be surrounded by the most thriving microbrew scene around.
And we’ve even got a campfire for nightime chats with professional athletes and experts.
So like we said, its just like summer camp when you were a kid.
The REP tri camp was born out of a simple idea. Build the best possible experience for our athletes. Period.
Knowledge. Tools. Decades of and coaching and clinical experience. Passion.
Thus summer, take your body to a whole different level.
Today in PT is a magazine for the physical therapy profession. They wrote:
Americans are increasingly on the run, with Running USA’s 2012 State of the Sport report counting nearly 39 million runners. Runners spend nearly $2.5 billion annually on footwear, according to the report. But, unfortunately, new shoes don’t come with accurate information and proper training to safely and successfully pursue the activity. For that, Today in PT turned to Jay Dicharry, PT, MPT, SCS, author of “Anatomy for Runners: Unlocking Your Athletic Potential for Health, Speed, and Injury Prevention.” click here for the rest
They threw out 10 questions, and i threw out 10 answers. Check out the link if you’d like to see some of the reasons why i do what I do, a few lines on the book, and why i got into this aspect of athletic injury care in the first place.
Multisport athletes have a lot of challenges in their training, but the training demands of 3 sports seem to creep up on all of us. Athletes spend so much time trying to fit in their volume that the body often gets ignored.
Well, this all ends now. Join me at the University of Michigan April 20-21st where we discuss “Putting the Athlete in Triathlete: a clinician’s role in endurance sports.” During this 13 hrs course, we’ll lay the ground work and discuss how endurance training impacts the tissues of the body, and then move on to detailed descriptions of the mechanics of each sport. You’ll learn how to correlate your musculoskeletal evaluation of the body with a runner’s swim, bike, and running performance. We’ll discuss why swimmers aren’t your typical overhead athletes, you’ll learn how to do bike fits (how to fit the bike to the rider, and more importantly how to fit the rider to the bike) with hands on practice, learn how to identify common gait patterns and cue them out of problems that overload the body, and understand the role of complimentary training and strengthening. At the end of the weekend, you’ll understand how to help your athletes make training easier on their body, and improve their efficiency.
for registration information, click here, and for a hourly breakdown of the course, click here. See you there!
What happens when you get 220+ clinicians in the room and talk about running? It was a beautiful day. About 55 degrees and sunny. The remnants of the 10+ in snowstorm on the ground helped dampen the air and made the sun feel even stronger. It’s a beautiful day for a run….but instead,about 220 clinicians sat inside, on their glutes, so they can learn to help you use your glutes better.
The 10th anniversary of the longest running, running specific medical conference produced a host of content to help “us” help “you.” Do you ever wonder why running is as challenging as it is? How your running would change if you had no gravity to fight, arms to swing, or perhaps even legs to stand on? Dr Rodger Kram led us in 2 enlightening presentations on the energetics of gait. Talks like this completely shift how you think about running.
Dr. Eric Carson reviewed the current and future trends on cartilage repair. Take home: right now, cutting edge surgeons are able to offer some pretty incredible proceedures, and they’ll be even more magic to come in the future.
Brian Hoke, PT helped us think critically through our video gait analysis. Anyone can watch a video in slow motion, but learning what to look for is critical.
Your’s truly helped clinicians through their musculoskeletal exams as they relate to a runner’s needs. No one can tlak about “correct running form” unless you understand that each runner is an individual with unique needs and attributes. If you understand how a person’s body wants to work, you can understand how to help that person run. For those of you who read the screen’s in Anatomy for Runners, that 8-point exam just got a whole lot more thorough: 32-points to be exact.
Dr Sibohn Stattua reviewed the literature on the female athlete triad. Turns out that there is more to it than just low energy intake, menstrual irregularity, and poor bone remodeling…..the triad is turning into a square? That’s right, there is a 4th “leg” to the triad, and this one might be even more severe of a long term complication from this complex disorder.
Eric Magrum, PT discussed the current research on the #1 injury affecting runners: anterior knee pain. He told us why runners with chronic pain in the knee try to avoid their pain. The problem is that the compensations we adopt to avoid pain in the knee are just as much of a problem as the original cause itself.
Kyle Kiesel, PhD, PT helped us through an eval process to identify core imbalances that affect far more than just the core.
And finally, Dr Bob Wilder guided us through the process of guiding you back to your running in explaining the best return to run programs after an injury.
Clinicans getting to know their feet: a scene from our lab session
And that doesn’t even mention the incredible lab session on Saturday by Brian Hoke, Kyle Kiesel, Dr Mark Cuccuzzella, myself, and the amazing cookies that I ate at the afternoon break. Egos were dropped at the door, and we all got down to the same level to help runners do what they love: run.
One of my favorite things is teaching. Sure I like the human body and what its capable of, but more importantly, I like the challenge of trying to teach average-Joe runner, their college coach, and their physicians and therapists. Each of these groups has a different education, different background, and different expectations, but they all want to learn to be better. Its my hope that I can offer some specific help to all of them.
I went to a class on teaching once, and learned a thing or 5000 about how we absorb and interpret information. To really enable someone to learn, you had to challenge the student to the point that their previous thought process is shattered. By poking holes in what we think, and replacing them with what we know, your and frame of understanding is shifted forever. Its my job to get you to think critically, so that you can think for yourself.
Since I get lots of people asking when my next talk is, I thought I’d share a few upcoming events in case folks were interested. Always good to cram more stuff in you brain.
Wed Dec 5th, 2013: The Running Event in Austin, TX – the annual conference for the Independent Running Retailer Association. Saucony is gracious enough to bring me in to discuss the mechanics of running. The more your local running retail staff knows about running the more they’ll be able to help you. I’ll also be doing book signings if anyone needs stocking stuffer.
Jan 20-21st, 2013: The Speed Summit in Morristown, NJ, an official USATF Level 3 Coaching Education Seminar. Want to save a few bucks? During checkout, type in “Dicharry” in the code box and you’ll save $10. Also if you print out the form and mail it in, you’ll also save an extra $9 dollar processing fee. I’ll be giving two talks: “How to prepare the body for optimal speed and strength training” and “How to screen for zebras in a field of horses.” But enough about me though….there are some major heavy hitters speaking. I’m really looking forward to this event.
Feb 23rd-24th, 2013: The Running Summit in Costa Mesa, CA, an official USATF Level 3 Coaching Education Seminar. And if you decide to attend, type in “Jay” in the code box during your checkout and you’ll save $10 dollars. An impressive weekend of discussion from some of the country’s most prominent coaches. As for me, I’ll be giving two talks: “Stretching, Strengthening, and Screening: Answers to questions to help your runners run” and “How shoes impact your form and how your form impact your shoes”
March 8-9th, 2013: The 10th Annual UVA Running Medicine Conference: From the Lab to the Clinic. This one really is near and dear to me. This started as a vision a decade ago when Founding-board members Dr. Robert Wilder, Eric Magrum, and myself came together to see what would happen if we had the first running-only medical education conference. Well, what began with 50 people mushroomed to over 240 of the most passionate running-specific healthcare providers in North America gathering to discuss better care for their patients. Its our 10th year! Thanks to all of you for your support over the years as we aim to give you the best experience possible. I’ll present “What to expect when you’re expecting: how clinical lab measures translate to gait.” But don’t come just for my talk! We’ve got a host of talented presenters, including the one and only Dr. Rodger Kram from CU-Boulder. Whenever I get some great brainwave creep into my head that I think is new, I’ll research it and sure enough, Dr Kram already found it out years ago. He’s brilliant and an amazing presenter that we are luck to have. And yes -there is a lab session yet again on Saturday and space is limited. Check out the link for full content.
April 19th and 20th: Care for the Injured Cyclist in Ann Arbor, MI. Yes, time to switch gears – literally. We’ll delve into the finer points of bike fit from both the performance and injury aspect, discuss how cycling contributes to chronic problems, and cover novel ways to improve on-the-bike stabilization and technique drills for efficiency. Don’t have the reg link for this one yet, but I’ll post it when I do.
Whew. that’s a lot for now. And somewhere in here, I need to fit in a ski trip!